NYACP Board Review Question of the Week
![]()
Every other Tuesday, NYACP members are sent a Board Review Question from ACP's MKSAP 18 to test professional knowledge and help prepare for the exam. Participant totals and answer percentages are distributed on the first Thursday of the month in IM Connected, the Chapter's eNewsletter, and are also published on this page.
If you are interested in receiving these questions bi-weekly, join us as a member!
If you are a member who needs to receive the questions and newsletter via email, let us know!
July 28th, 2026
MKSAP 19 Nephrology, Question 80
A 45-year-old woman is evaluated in the emergency department for altered mental status.
On physical examination, the patient is tachypneic and obtunded. Temperature is normal, blood pressure is 94/64 mm Hg, pulse rate is 80/min, and respiration rate is 24/min.
|
Laboratory studies: |
|
|
Electrolytes: |
|
|
Sodium |
133 mEq/L (133 mmol/L) |
|
Potassium |
3.9 mEq/L (3.9 mmol/L) |
|
Chloride |
110 mEq/L (110 mmol/L) |
|
Bicarbonate |
16 mEq/L (16 mmol/L) |
|
Arterial blood gases: |
|
|
pH |
7.4 |
|
PCO2 |
27 mm Hg (3.6 kPa) |
Which of the following is the most likely acid-base disorder?
A. Respiratory alkalosis and increased anion gap metabolic acidosis
B. Respiratory alkalosis and normal anion gap metabolic acidosis
C. Respiratory alkalosis, normal gap metabolic acidosis, and metabolic alkalosis
D. Respiratory alkalosis with chronic compensation
Responses Received from Members (997 Responses):
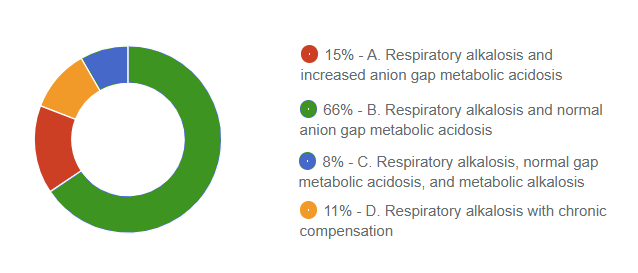
The Correct Answer is: B. Respiratory alkalosis and normal anion gap metabolic acidosis
Educational Objective: Diagnose a mixed acid-base disorder.
The most likely acid-base disorder is a respiratory alkalosis and normal gap metabolic acidosis (Option B). The first step in the interpretation of acid-base disorders usually requires the identification of the likely dominant or primary acid-base disorder, followed by an assessment of the compensatory response. When measured values fall outside the expected compensatory range, a mixed acid-base disorder is considered present. The primary disorder is usually reflected by the blood pH. Appropriate compensation may result in near-normal pH but never a normal pH. In patients with an obvious acid- base disturbance (for example, an abnormal serum bicarbonate), a normal pH suggests the presence of a mixed acid-base disorder. In this case, the patient's pH of 7.4 does not allow for a clear assignment of the primary disorder and therefore indicates a mixed acid-base disorder. The patient has a PCO2 of 27 mm Hg (3.6 kPa), suggesting the presence of a respiratory alkalosis. The expected metabolic compensation for chronic respiratory alkalosis is a reduction in the serum bicarbonate of 4 to 5 mEq/L (4-5 mmol/L) for each 10 mm Hg (1.3 kPa) decrease in the PCO2. In this case, the decrease in PCO2 is 13 mm Hg (1.7 kPa); thus, the serum bicarbonate is expected to be 5.2 to 6.5 mEq/L (5.2- 6.5 mmol/L) lower than normal. Therefore, expected serum bicarbonate would be calculated as follows:
Normal Bicarbonate − Expected Compensation
24 − (5.2-6.5) mEq/L (mmol/L) = 17.5-18.8 mEq/L (17.5-18.8 mmol/L)
The patient's serum bicarbonate of 16 mEq/L (16 mmol/L) is lower than expected, indicating the presence of a concurrent metabolic acidosis. The anion gap of 7 is normal, indicating a normal anion gap metabolic acidosis.
Respiratory alkalosis with an increased anion gap metabolic acidosis (Option A) is not correct because the anion gap is 7, and thus not exceeding the normal threshold of 8.0 to 10 mEq/L ± 2.0 mEq/L (8.0- 10 mmol/L ± 2.0 mmol/L).
Respiratory alkalosis, normal anion gap metabolic acidosis, and metabolic alkalosis (Option C) is not correct because the serum bicarbonate is lower, not higher, than the expected compensatory response.
Respiratory alkalosis with chronic compensation (Option D) is partially correct but does not account for the serum bicarbonate level being lower than the expected compensatory response, which indicates a concurrent metabolic acidosis.
Key Points
- The first step in the interpretation of acid-base disorders requires the identification of the likely dominant acid-base disorder, followed by an assessment of the compensatory response.
- In the interpretation of acid-base disorders, when measured values fall outside the expected compensatory range, a mixed acid-base disorder is present.
Bibliography
Seifter JL, Chang HY. Disorders of acid-base balance: new perspectives. Kidney Dis (Basel). 2017;2:170-186. PMID: 28232934 doi:10.1159/000453028
Multiple-choice questions reprinted with permission from the American College of Physicians.
MKSAP 19. © Copyright 2021 American College of Physicians.
ACP MKSAP. © Copyright 2026 American College of Physicians. All Rights Reserved All Rights Reserved.
July 14th, 2026
MKSAP 19 Oncology, Question 57
A 53-year-old man is evaluated in the office following hemicolectomy for adenocarcinoma of the colon. He is otherwise healthy, has no symptoms, and takes no medications.
Physical examination is normal.
Presurgical contrast-enhanced CT scan of the chest, abdomen, and pelvis was negative for metastases.
Pathology revealed a 4-cm adenocarcinoma that was poorly differentiated and invading into the submucosa but not into the muscularis. All 17 lymph nodes sampled were negative for tumor. The tumor is staged as T2N0 (stage I). The tumor is negative for KRAS, NRAS, and BRAF mutations.
Which of the following is the most important prognostic factor?
A. Degree of tumor differentiation
B. KRAS, NRAS, and BRAF tumor mutational status
C. Performance status of patient
D. Size of the tumor
E. Stage of the tumor
Responses Received from Members (1158 Responses):
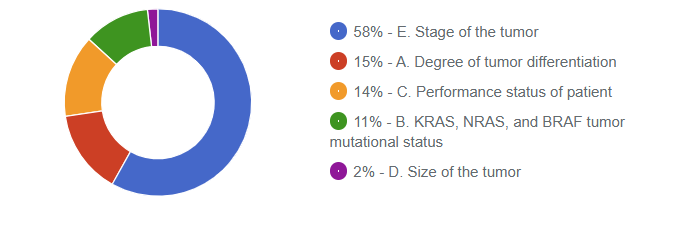
The Correct Answer is: E. Stage of the tumor
Educational Objective: Evaluate cancer prognosis.
Tumor stage (Option E) is usually the most important prognostic factor in determining a patient's outcome. All tumors are staged using the American Joint Commission on Cancer staging system. This involves the TNM system, in which the extent of the tumor (size and/or depth of penetration), nodes (number of local-regional nodes that contain cancer), and metastases (present or absent) are considered. TNM scorings are placed on a scale of stage I though IV, with stage 1 having the best prognosis and stage IV the worst.
Poorly differentiated tumors (Option A) have, in general, a worse prognosis than well-differentiated tumors; however, this too is a modest prognostic factor compared with staging.
Although molecular profiling for driver mutations in genes such as KRAS, NRAS, and BRAF (Option B) may influence prognosis and may have implications for chemotherapy selections in advanced disease, they have far less influence on outcome than tumor stage. In addition, they are not relevant in the management of stage I colon cancer, which has a very favorable prognosis and would not require further therapy after surgery.
Performance status (Option C), which is a designation of the overall medical wellness, or lack thereof, of the patient may have important prognostic implications within a particular stage of disease but is far less significant prognostically than the staging itself. It is important to differentiate patients with a poor performance status who are debilitated due to chronic comorbidities from patients who would otherwise be medically fit but are acutely debilitated by their cancer. The latter situation may warrant an attempt at aggressive treatment because reversing the cancer process is the only option that will improve the patient's overall condition, whereas the former may need to be treated with. less aggressive treatment or possibly no specific anticancer treatment.
Tumor size (Option D) may be a component of the “T” stage, but by itself, it has only modest prognostic significance relative to overall stage.
Key Point
- Staging is generally the most accurate prognostic indicator and largely dictates the therapeutic strategy for patients with cancer.
Bibliography
Daly MC, Paquette IM. Surveillance, epidemiology, and end results (SEER) and SEER-medicare databases: use in clinical research for improving colorectal cancer outcomes. Clin Colon Rectal Surg. 2019;32:61-68. PMID: 30647547 doi:10.1055/s-0038-1673355
Multiple-choice questions reprinted with permission from the American College of Physicians.
MKSAP 19. © Copyright 2021 American College of Physicians.
ACP MKSAP. © Copyright 2026 American College of Physicians. All Rights Reserved All Rights Reserved.