NYACP Board Review Question of the Week
![]()
Every other Tuesday, NYACP members are sent a Board Review Question from ACP's MKSAP 18 to test professional knowledge and help prepare for the exam. Participant totals and answer percentages are distributed on the first Thursday of the month in IM Connected, the Chapter's eNewsletter, and are also published on this page.
If you are interested in receiving these questions bi-weekly, join us as a member!
If you are a member who needs to receive the questions and newsletter via email, let us know!
August 11th, 2026
MKSAP 19 General Internal Medicine 1, Question 23
A 56-year-old man is evaluated during a routine follow-up appointment. He has schizophrenia treated with olanzapine. Currently, the patient experiences no hallucinations or delusions. He is otherwise healthy. Previous ECGs have been normal.
On physical examination, vital signs are normal. BMI is 27. The examination shows flat affect. Speech is normal, and thoughts appear organized.
A fasting blood glucose measurement is pending.
Which of the following should also be monitored in this patient?
A. Complete blood count
B. Lipid levels
C. Liver chemistries
D. Prolactin level
E. QT interval
Responses Received from Members (Graph is uploaded on Thursday afternoon):
The Correct Answer is: B. Lipid levels
Educational Objective: Monitor a patient taking antipsychotic medication.
Lipid levels (Option B), weight, and blood glucose level should be monitored in this patient who has schizophrenia and takes olanzapine, a second-generation antipsychotic medication. Schizophrenia is associated with an increased risk for diabetes mellitus, cardiovascular disease, and obesity, and undertreatment of medical disease is common in this population. Metabolic effects of antipsychotic therapy also can contribute to these conditions, which significantly increase mortality in patients with schizophrenia. The most common adverse effects of second-generation antipsychotic agents are weight gain (and sequelae of weight gain, such as hyperglycemia) and hyperlipidemia. The fasting blood glucose level should be measured upon initial medication initiation and at 3 months.
Thereafter, the fasting glucose level should be checked at least annually. More frequent monitoring can be considered in patients with risk factors for diabetes. Lipid monitoring should be performed at baseline, at 3 months, and at least every 5 years thereafter.
Complete blood count monitoring (Option A) is required for patients who take clozapine owing to its association with agranulocytosis. Routine complete blood count monitoring is not required with olanzapine use.
Periodic monitoring of liver chemistries (Option C) is required with use of some first-generation antipsychotics, such as fluphenazine, but it is not needed with olanzapine.
First-generation (typical) antipsychotic agents have a higher risk for extrapyramidal symptoms (parkinsonism, akathisia), tardive dyskinesia, and hyperprolactinemia than do second-generation (atypical) antipsychotic agents. Regardless of whether the patient is treated with typical or atypical agents, in the absence of side effects, such as nipple discharge, routine monitoring of the prolactin level (Option D) is not indicated.
Second-generation antipsychotic agents, including olanzapine, have been associated with a prolonged QT interval. However, the incidence of prolonged QT interval with olanzapine alone is less than 2%. When combined with other agents that can prolong the QT interval (quinidine, selective serotonin reuptake inhibitors, tricyclic antidepressants, ondansetron), QT should be monitored. In a patient with a previously normal QT interval and no new medications, routinely obtaining an ECG for QT interval monitoring (Option E) is not required.
Key Points
- The most common adverse effects of second-generation antipsychotic agents are weight gain (and sequelae of weight gain, such as hyperglycemia) and hyperlipidemia.
- Weight, blood glucose level, and lipid levels should be monitored in patients taking second- generation antipsychotic drugs.
Bibliography
American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601. PMID: 14747245 doi:10.2337/diacare.27.2.596
Multiple-choice questions reprinted with permission from the American College of Physicians.
MKSAP 19. © Copyright 2021 American College of Physicians.
ACP MKSAP. © Copyright 2026 American College of Physicians. All Rights Reserved All Rights Reserved.
July 28th, 2026
MKSAP 19 Nephrology, Question 80
A 45-year-old woman is evaluated in the emergency department for altered mental status.
On physical examination, the patient is tachypneic and obtunded. Temperature is normal, blood pressure is 94/64 mm Hg, pulse rate is 80/min, and respiration rate is 24/min.
|
Laboratory studies: |
|
|
Electrolytes: |
|
|
Sodium |
133 mEq/L (133 mmol/L) |
|
Potassium |
3.9 mEq/L (3.9 mmol/L) |
|
Chloride |
110 mEq/L (110 mmol/L) |
|
Bicarbonate |
16 mEq/L (16 mmol/L) |
|
Arterial blood gases: |
|
|
pH |
7.4 |
|
PCO2 |
27 mm Hg (3.6 kPa) |
Which of the following is the most likely acid-base disorder?
A. Respiratory alkalosis and increased anion gap metabolic acidosis
B. Respiratory alkalosis and normal anion gap metabolic acidosis
C. Respiratory alkalosis, normal gap metabolic acidosis, and metabolic alkalosis
D. Respiratory alkalosis with chronic compensation
Responses Received from Members (997 Responses):
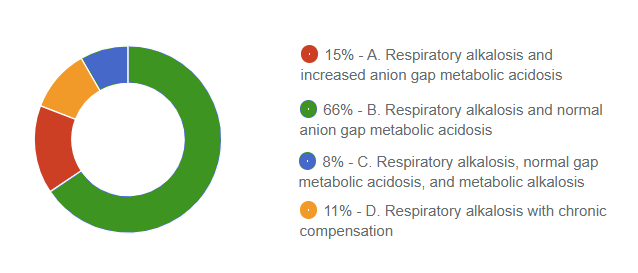
The Correct Answer is: B. Respiratory alkalosis and normal anion gap metabolic acidosis
Educational Objective: Diagnose a mixed acid-base disorder.
The most likely acid-base disorder is a respiratory alkalosis and normal gap metabolic acidosis (Option B). The first step in the interpretation of acid-base disorders usually requires the identification of the likely dominant or primary acid-base disorder, followed by an assessment of the compensatory response. When measured values fall outside the expected compensatory range, a mixed acid-base disorder is considered present. The primary disorder is usually reflected by the blood pH. Appropriate compensation may result in near-normal pH but never a normal pH. In patients with an obvious acid- base disturbance (for example, an abnormal serum bicarbonate), a normal pH suggests the presence of a mixed acid-base disorder. In this case, the patient's pH of 7.4 does not allow for a clear assignment of the primary disorder and therefore indicates a mixed acid-base disorder. The patient has a PCO2 of 27 mm Hg (3.6 kPa), suggesting the presence of a respiratory alkalosis. The expected metabolic compensation for chronic respiratory alkalosis is a reduction in the serum bicarbonate of 4 to 5 mEq/L (4-5 mmol/L) for each 10 mm Hg (1.3 kPa) decrease in the PCO2. In this case, the decrease in PCO2 is 13 mm Hg (1.7 kPa); thus, the serum bicarbonate is expected to be 5.2 to 6.5 mEq/L (5.2- 6.5 mmol/L) lower than normal. Therefore, expected serum bicarbonate would be calculated as follows:
Normal Bicarbonate − Expected Compensation
24 − (5.2-6.5) mEq/L (mmol/L) = 17.5-18.8 mEq/L (17.5-18.8 mmol/L)
The patient's serum bicarbonate of 16 mEq/L (16 mmol/L) is lower than expected, indicating the presence of a concurrent metabolic acidosis. The anion gap of 7 is normal, indicating a normal anion gap metabolic acidosis.
Respiratory alkalosis with an increased anion gap metabolic acidosis (Option A) is not correct because the anion gap is 7, and thus not exceeding the normal threshold of 8.0 to 10 mEq/L ± 2.0 mEq/L (8.0- 10 mmol/L ± 2.0 mmol/L).
Respiratory alkalosis, normal anion gap metabolic acidosis, and metabolic alkalosis (Option C) is not correct because the serum bicarbonate is lower, not higher, than the expected compensatory response.
Respiratory alkalosis with chronic compensation (Option D) is partially correct but does not account for the serum bicarbonate level being lower than the expected compensatory response, which indicates a concurrent metabolic acidosis.
Key Points
- The first step in the interpretation of acid-base disorders requires the identification of the likely dominant acid-base disorder, followed by an assessment of the compensatory response.
- In the interpretation of acid-base disorders, when measured values fall outside the expected compensatory range, a mixed acid-base disorder is present.
Bibliography
Seifter JL, Chang HY. Disorders of acid-base balance: new perspectives. Kidney Dis (Basel). 2017;2:170-186. PMID: 28232934 doi:10.1159/000453028
Multiple-choice questions reprinted with permission from the American College of Physicians.
MKSAP 19. © Copyright 2021 American College of Physicians.
ACP MKSAP. © Copyright 2026 American College of Physicians. All Rights Reserved All Rights Reserved.